ACLS
Last week I joined a training on ACLS: Advanced Cardiology Life Support. My joining this was partly because I need the certification, but for the most part because I dreaded cardiology cases. When I dreaded something, I tend to be attracted more to it. I need to know more. I came at the first day of the course with determination still undecided. I still thought that my attending ACLS course was a mistake. I hated cardiology. But then, after 3 days of lots and lots of theory were crammed into our tiny heads and a lot more practices (my body actually ached because of all those chest compression I did), I am ready to sell my soul to cardiology. I loved it! Or probably it's just because I like being in stressful conditions. Soon I would be a typical patient for ACLS. Well, hopefully not.
ACLS was only one of the certifications an emergency care practitioner should have. Although recently I heard that PDKI (Persatuan Dokter Keluarga Indonesia = The Indonesian Association of Family Physicians) wanted all doctors (who the association considered as family physicians) to have ACLS and ATLS (Advanced Trauma Life Support) certifications, which are not cheap at all, oh no, mam. Each year it's getting more and more expensive.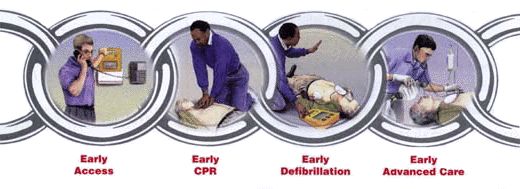 ACLS is a detailed medical protocol for the provision of lifesaving cardiac care in setings ranging from pre-hospital environment to the hospital setting. There are a lot of algorithms in ACLS, but the most important algorithms are for ventricular fibrillation (VF), pulseless ventricular tachycardia (pulseless VT), asystole, pulseless electrical activity (PEA), and acute coronary syndrome (ACS).
ACLS is a detailed medical protocol for the provision of lifesaving cardiac care in setings ranging from pre-hospital environment to the hospital setting. There are a lot of algorithms in ACLS, but the most important algorithms are for ventricular fibrillation (VF), pulseless ventricular tachycardia (pulseless VT), asystole, pulseless electrical activity (PEA), and acute coronary syndrome (ACS).
ACLS consists of 4 chain links:
- early recognition and access: when one established the unresponsiveness of a patient, bystander called emergency services like 911.
I don't remember what is the emergency number in Indonesia, but mostly it didn't respond. You know how Indonesian health services are. In Banjarmasin, ambulance is just a car with reversed "ambulance" letters written in front, without any medical emergency appliances in there, let alone the health providers. The driver is a layman who had no basic training in first aid whatsoever. So you can imagine what would happen to someone with broken neck. Or someone with broken leg. Or someone with VF. There's a lot of mortality happened outside the hospital. - early CPR: CPR as in cardiopulmonary resuscitation. Compress the heart and assist breathing. Common people in US (and maybe in EUrope, too) are familiar to BLS (basic life support: make sure airway is open, assist breathing by mouth-to-mouth, compress the heart), so this link is still performed by people on the street. When you feel no pulse and saw no breathing, you start CPR.
What we do in Indonesia? Just stand around the patient in safe distance, while some people's calling police or ambulance (which usually not coming, and if it's come, it won't bring any help anyway), until one good soul will offer his/her car to bring the patient to the hospital. And maybe at that time it's already too late. Early help is the most important point that will decrease the mortality of cardiac arrest. - early defibrillation: this is the most awesome part. In US, and Europe, there is this automated external defibrillator (AED) set everywhere, especially at places with >250 adults over 50 years of age present for >16 hours/day. I even read somewhere that even international airplanes have this AED aboard. What AED do? It brings back the fatal irregular rythm called VF to its regular rhytm. It was said that early fibrillation (prehospital) will double the VF survival rate. The best part is this: laymen can do the defibrillation. AED was designed so that when lay rescuer attach the AED to the chest of the patient, it will immediately diagnose if the patient had VF or not, and then it will prompt the rescuer to do the defibrillation. A very good concept.
Now, can we do the same in Indonesia? No, we can't, poor us. The day you put AEDs in railway stations or airplanes or shopping malls, that is the day you will see the last of them (OK, I am being hyperbolic here). Even phonebooths do not work out in our country, being stolen or damaged. Hell, even cables and iron bars of a bridge were stolen. A lot more people will be dead because of undiagnosed, and untreated, VF. - early ACLS: this is when the ACLS team come, the ones who are trained in cardiology life support. Or it could means when the patient arrived at the hospital, while CPR continued in ambulance.
There are not many health providers in Indonesia trained in ACLS. Not all considered it important, I guess, except when he/she worked in emergency care or intensive care. Besides, the training cost is Rp 2.500.000 (on May 2006). Doctors are more interested in ATLS, which engaged more with trauma life support (although the cost is more expensive: Rp 4.000.000). Besides, as far as I know, ACLS training is given only to doctors, which is wrong. If you saw in Chicago Hope or ER, ambulance drivers, nurses, and doctors are all skilled in emergency care and seemed like they work along a rule or a code, they seemed to know things to do without being prompted to. I read in someone's blog that in US, ACLS training is given to doctors and nurses alike. And the blogger admitted that the nurses are even more skilled than she is (she is a doctor) in reading the ECG monitor and deciding which algorithms to take. Makes you think again about your medical education method back in medschool, isn't it?
The tutor for my 3-days ACLS training was from UI Jakarta (dr Agus), Surabaya (dr Samuel), Solo (dr Ninik), Jogja (dr Nahar), and Semarang (dr Bambang). The tutors were cardiologists specially trained to be a tutor in ACLS. Seeing from the high cost of the mannequins, equipments, maintenances, transportation of all those, I think the training cost is too cheap. The trainers must be very dedicated. They have to sacrifice 2 days of their practices. They said that seeing their students come on the first day with almost-zero skill of ACLS and leaving at third day more than 80% skilled is the most rewarding thing they get.
posted by mina @ 11:45 PM
![]() Del.icio.us
Del.icio.us




2 Comments:
At 10/21/2006 04:22:00 AM
I recently published an article on drug rehab – here is a quote from it, in case you are interested:
Statistics give us more and more pieces of information that are bound to worry us, to make us react and change something if we can. More and more people and in earlier and earlier stages of their life die of a heart disease. Statistics, only in the US, are extremely alarming:
- Every 30 seconds someone dies because of a heart disease;
- More than 2.500 Americans die daily because of heart diseases;
- Every 20 seconds there is a person dying from a heart attack;
- Each year 6 million people are hospitalized because of a heart disease;
- The number 1 killer is a heart disease.
Although AEDs are not a universal panacea for all heart diseases, nothing else can compete to its major feature, that of actually re-starting the heart after it has been stopped by a sudden cardiac arrest. Under these circumstances is it necessary to ask you why anyone in this world, any family, in any home would hope for having such a device in their first aid locker?
If you feel this help, please drop by my website for additional information, such as Public Access Defibrillatio PAD or additional resources on AED manufacturers such as Philips defibrillators, Zoll AEDs or Cardiac Science AEDs.
Regards,
Michael
Posted by Michael Rad
At 4/20/2013 09:31:00 PM
Hi there, I read your new stuff on a regular basis. Your writing style is awesome, keep doing what you're doing!
my web-site - Http://Encyklopediaverbena.pl/